Bilateral superior semicircular canal dehiscence - A rare cause of disequilibrium and pulsatile tinnitus
DOI:
https://doi.org/10.34631/sporl.78Keywords:
Superior semicircular canal dehiscence, autophonia, oscillopsia, dizziness, vestibular-evoked myogenic potentials, diagnosis, treatmentAbstract
Introduction: Superior semicircular canal dehiscence syndrome (SSCDS) is a recently recognized clinical condition which was initially described by Minor et al. in 1998. The proposed underlying mechanism involves the existence of a dehiscence of bone overlaying the superior semicircular canal creating a third mobile window which produces a path of least resistance that shunts acoustic energy through the vestibular labyrinth rather than through the cochlea. This syndrome may present with various symptoms such as sound or pressure induced vertigo (Tullio phenomenon) and oscillopsia along with hearing loss, autophony or tinnitus. It typically manifests as sound and/or pressure induced nystagmus at the plane of the SSC (vertical-torsional eye movements).
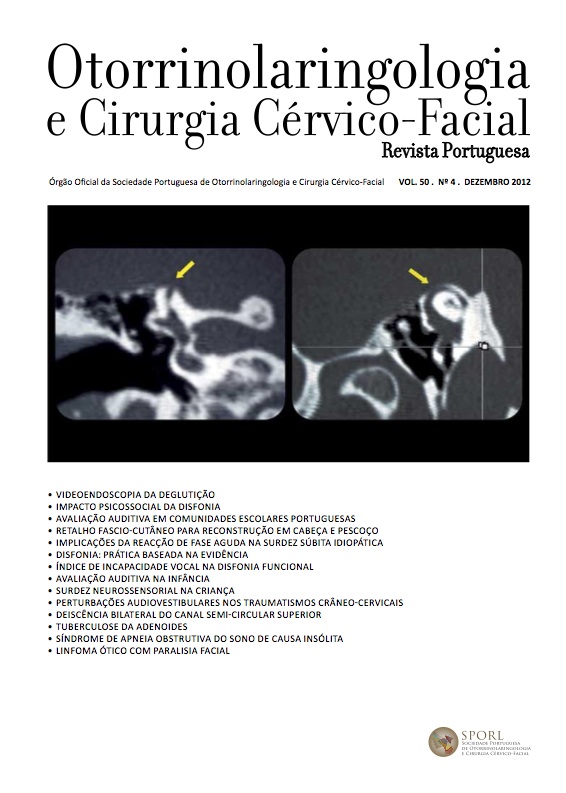
Subjects and methods: The authors report a case of bilateral superior semicircular canal dehiscence presenting with left pulsatile tinnitus and disequilibrium and demonstrate the clinical utility of vestibular-evoked myogenic potentials (VEMP) in the diagnosis of this unusual and underdiagnosed clinical entity.
Results: Diagnosis is based on the correlation of clinical symptoms, audiologic and vestibular testing and highresolution CT scan. Audiometric findings include low-frequency air-bone gap with preservation of acoustic reflexes. The most specific vestibular test available for SSCDS is VEMP testing. However, the established standard to confirm diagnosis is high-resolution temporal bone CT scan. Management of SSCDS is directed at symptom control and in many cases no treatment is required, besides reassurance and avoidance of the precipitating stimuli. Surgical repair is reserved for patients with disabling symptoms.
Conclusion: SSCDS is a rare disease and probably underdiagnosed. However, not all patients with a diagnosis of SSCDS will have classic symptoms and signs. A high index of suspicion with careful clinical examination and audiologic testing is required to identify these patients. VEMP testing can be very useful in diagnosing these patients.
Downloads
References
Minor L, Solomon D, Zinreich J, Zee D. Sound and/or pressure induced vertigo due to bone dehiscence of the superior semicircular canal. Arch Otolaryngol Head Neck Surg. 1998; 124: 249-258.
Carey J, Minor L, Nager T. Dehiscence or thinning of bone overlying the superior semicircular canal in a temporal bone survey. Arch Otolaryngol Head Neck Surg. 2000; 126: 137-147.
Williamson R, Vrabec J, Coker N, Sandlin M. Coronal computed tomography prevalence of superior semicircular canal dehiscence. Otolaryngol Head Neck Surg. 2003; 129: 481-489.
Branstetter B, Harrigal C, Escott E, Hirsch B. Superior semicircular canal dehiscence: oblique reformatted CT images for diagnosis. Radiology. 2006; 238: 938-942.
Minor L. Clinical manifestations of superior semicircular canal dehiscence. Laryngoscope; 115: 1717- 1727.
Banerjee A, Whyte A, Atlas. Superior canal dehiscence: review of a new condition. Clin Otolaryngol. 2005; 30: 9-15.
Watson S, Halmagyi G, Colebatch j. Vestibular hypersensitivity to sound (Tullio phenomenon): structural and functional assessment. Neurology. 2000; 54: 722-728.
Brantberg K, Bergenius J, Mendel L, Witt H, Tribukait A et al. Symptoms, findings and treatment in patients with dehiscence of the superior semicircular canal. Acta Otolaryngol. 2001; 121: 68-75.
Minor L. Superior canal dehiscence syndrome. Am J Otol. 2000; 21:9-19.
Minor J, Cremer P, Carey J, et al. Symptoms and signs of superior canal dehiscence syndrome; Ann N Y Acad Sci. 2001; 942: 259-273.
Laperrière S, Bertholon P, Chardon S, Prades J. Déhiscence du canal semi-circulaire supérieure. Fr ORL. 2006; 91: 249-256.
Bastian D, Tran Ba Huy P. Organogenèse de l’oreille moyenne. Encycl Méd Chir (Elsevier Paris), Oto-rhino-laryngologie, 20-005-A-30, 1996, p.6.
Brantberg K, Bergenius J, Tribukait A. Vestibular-evoked myogenic potentials in patients with dehiscence of the superior semicircular canal. Acta Otolaryngol (Stockh). 1999; 119: 633-640.
Curtin H. Superior semicircular canal dehiscence syndrome and multi-detector row CT. Radiology. 2003; 226 (2): 312-314.
RosowskiJ, Songer J, Nakajima H, Brinsko K et al. Clinical, experimental and theoretical investigations of the effect of superior semicircular canal dehiscence on hearing mechanisms. Otol Neurotol. 2004; 25: 323-332.
Minor L, Carey J, Lustig L, Streubel S et al. Dehiscence of bone overlying the superior canal as a cause of apparent conductive hearing loss. Otol Neurotol. 2003; 24: 270-278.
Streubel S, Cremer P, Carey J, Minor L et al. Vestibular-evoked myogenic potentials in the diagnosis of superior canal dehiscence syndrome. Acta Otolaryngol. 2001; Suppl 545: 41-49.
Brantberg K, Verrecchia L. Testing vestibular-evoked myogenic potentials with 90-dB clicks is effective in the diagnosis of superior canal dehiscence syndrome. Audiol Neurotol. 2009; 14: 54-58.
Roditi R, Eppsteiner R, Sauter T, Lee D. Cervical vestibular evoked myogenic potentials (cVEMPs) in patients with superior canal dehiscence syndrome (SCDS). Otolaryngol Head Neck Surg. 2009; 141:24-28.
Colebatch J, Halmagyi G, Skuse N. Myogenic potentials generated by a click-evoked vestibulocollic reflex. J Neurol Neurosurg Psychiatry. 1994; 57; 190-197.
Colebatch J, Day B, Bronstein A, Davies R, Luxon L et al. Vestibular hypersensitivity to clicks is characteristic of the Tullio phenomenon. J Neurol Neurosurg Psychiatry. 1998; 65: 670-678.
Belden J, Weg N, Minor L, Zinreich S. CT evaluation of bone dehiscence of the superior semicircular canal as a cause of sound and/or pressure-induced vertigo. Radiology. 2003.226: 337-343.
Phililips D, Souter M, VitkovitchJ, Briggs R. Diagnosis and outcomes of middle cranial fossa repair for patients with superior semicircular canal dehiscence syndrome. J Clin Neurosci. 2010; 17: 339-341.
Teixido M, Artz G, Kung B. Clinical experience with symptomatic superior canal dehiscence in a single neurotologic practice. Otolaryngol Head Neck Surg. 2008; 139: 405-413.