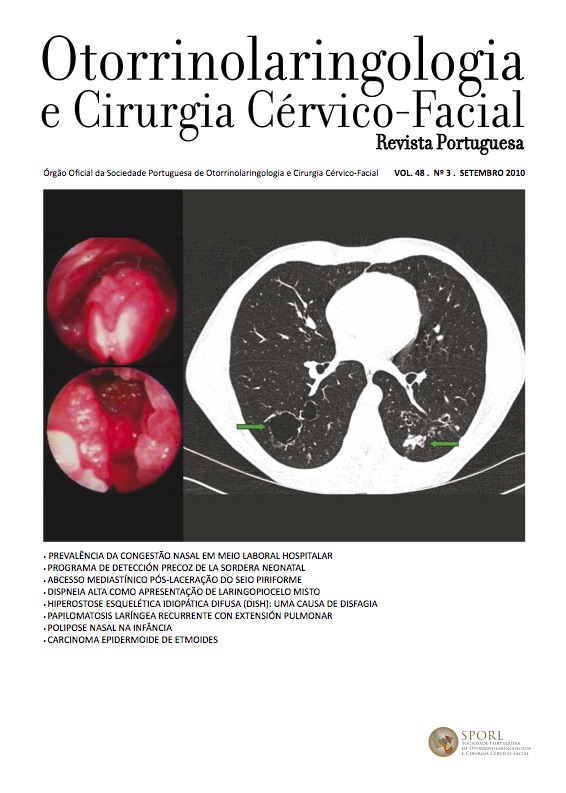
Mediastinal abscess following iatrogenic piriform fossa perforation - case report
DOI:
https://doi.org/10.34631/sporl.224Keywords:
Mediastinal abscess, Endotracheal intubation, Iatrogenic perforation, Pharyngoesophageal perforationAbstract
The hypopharynx and cervical oesophagus are particularly vulnerable areas of injury resulting from endotracheal intubation. These anaesthesia accidents are uncommon, rarely reported and its incidence is higher in the emergency situation. The pharyngoesophageal perforations may stay unnoticed until characteristic signs and symptoms are present, such as cervical pain, fever, dysphagia, leukocytosis, subcutaneous emphysema and pneumomediastinum. Surgical treatment vs conservative treatment is controversial. It is agreed, however, that the time interval between the initial trauma and diagnosis and treatment is the single most important factor affecting outcome. We report a case of mediastinal abscess following piriform fossa perforation occurring after a difficult intubation for an emergent caesarean delivery.
Downloads
References
Goudy SL, Miller FB, Bumpous JM. Neck Crepitance: Evaluation and management of suspected upper aerodigestive tract injury. Laryngoscope 2002;112:791-95.
Cameron JR, Kieffer RF, Hendrix TR, Mehigan DG, Baker RR. Selective nonoperative management of contained intrathoracic esophageal disruptions. Ann Thorac Surg 1979;27:404-8.
Michel L, Grillo HC, Malt RA. Operative and nonoperative management of esophageal perforations. Ann Surg 1981;194:56-63.
Tartell PB, Hoover LA, Friduss ME, Zuckerbraun L. Pharyngoesophageal intubation injuries: three case reports. Am J Otolaryngol. 1990 Jul-Aug; 11(4):256-60.
Shockley W, Tate J, Stucker F. Management of perforations of the hypo pharynx and cervical esophagus. Laryngoscope 1985; 95:939-941.
Sarr MD, Pemberton JH, Payne WS. Management of instrumental perforation of the esophagus. J Thorac Cardiovasc Surg 1982;84:211-8.
Pillay SP, Ward M, Cohen A, Pollard E. Oesophageal ruptures and perforations - a review. Med J Aust 1989;150:246-52.
Sanford RD, Narendra RK, Thomas WW, Anthony JM. Conservative medical management of traumatic pharyngoesophageal perforations. Ann Otol Rhinol Laryngol 1992;101:209-15.
Domino K, Posner K, Caplan R, Cheney F. Airway injury during anesthesia: a closed claims analysis. Anesthesiology 1999; 91:1703-1711.
Clayton J. Brinster, BA, Sunil Singhal, MD, Lawrence Lee, BS, M. Blair Marshall, MD, Larry R. Kaiser, MD, John C. Kucharczuk, MD. Evolving options in the management of esophageal perforation. Ann Thorac Surg 2004;77:1475-83.